
 Appointments
AppointmentsPatella Instability : Causes, Treatment, and Recovery
Patella instability — with Dr Lingaraj Krishna — is more common than many patients realise. The kneecap slips out of its groove, causing pain, swelling, and a feeling of giving way. For patella instability, Dr Lingaraj provides a clear diagnosis and a structured treatment plan before the condition worsens.
If your knee has felt unstable or “given way” before, this guide is for you. Read on to understand the causes, treatment options, and what recovery looks like.
What Is Patella Instability?
The patella (kneecap) sits in a groove at the front of the knee. Normally, it glides smoothly as you bend and straighten your leg. In patients with patella instability, the kneecap moves out of this groove. This is called subluxation (partial dislocation) or full dislocation.
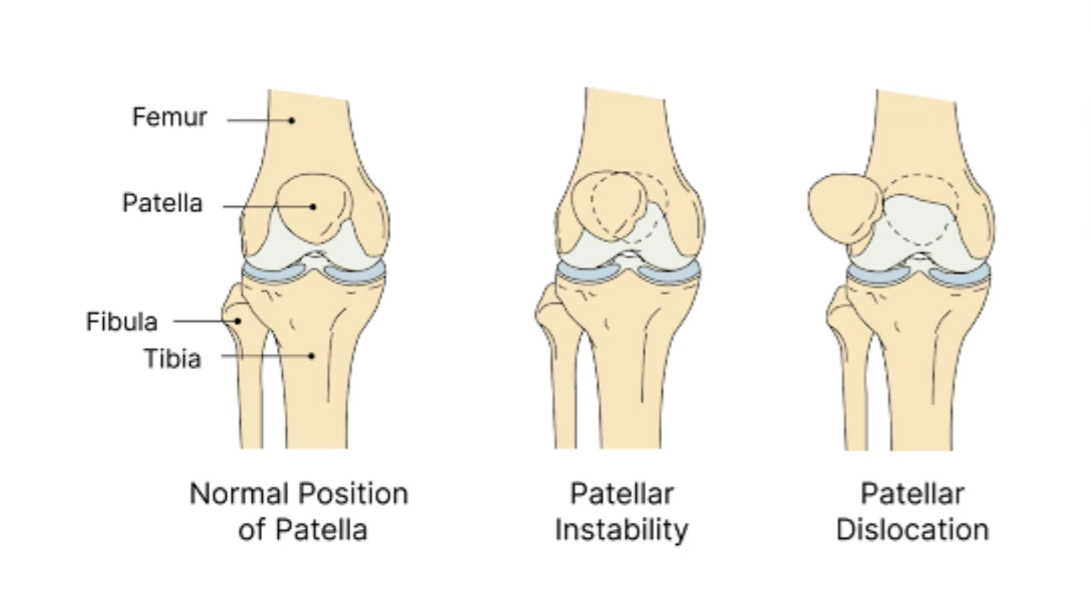
Patients often describe the sensation as the knee “giving way.” Some hear a pop. Others see visible swelling within hours. Dr Lingaraj explains that this is not simply a bruise — the knee has suffered real structural stress.
Who Is at Risk?
Patella instability affects people of all ages. However, certain factors raise the risk:
- Shallow groove: Some people are born with a trochlear groove that is too flat. This gives the kneecap less support.
- High-riding kneecap: Doctors call this “patella alta.” The kneecap sits too high and is less stable.
- Weak hip and thigh muscles: Poor muscle support allows the kneecap to drift sideways.
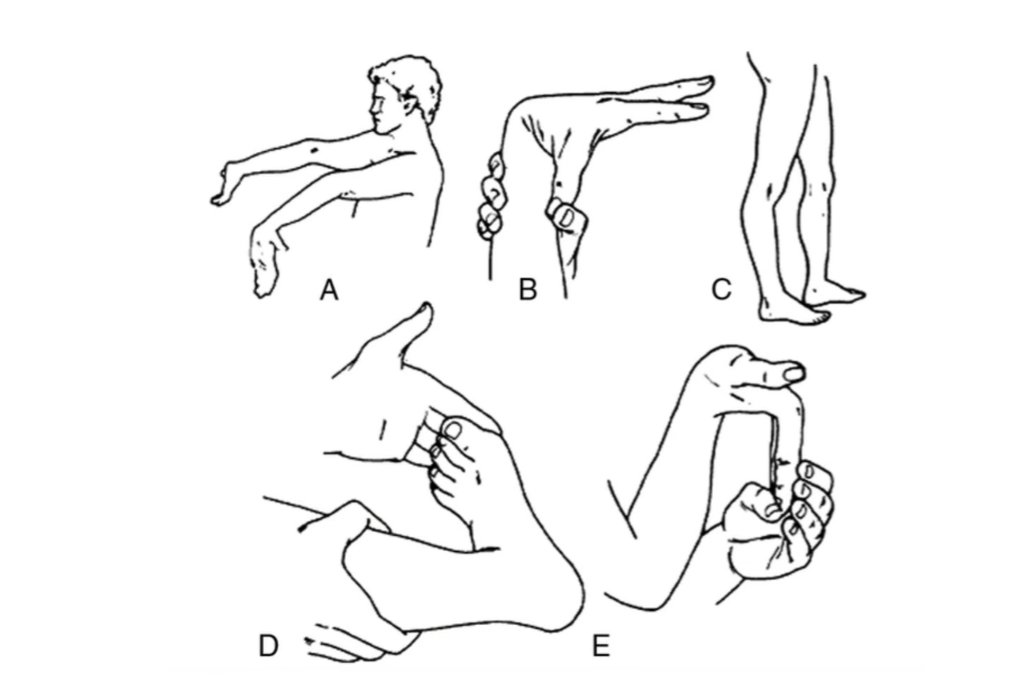
- Loose ligaments: Hypermobile joints increase the risk of dislocation.
- Previous dislocation: One dislocation increases the chance of another.
Young athletes and active teenagers are particularly vulnerable. Dr Lingaraj sees many adolescent patients who have dislocated their kneecap during sport and are unsure of the next step.
How Dr Lingaraj Diagnoses Patella Instability
Dr Lingaraj begins every assessment with a full history and physical examination. He asks about the mechanism of injury, whether the knee “popped out,” and how the patient managed it. He also checks for tenderness along the medial side of the knee — where the MPFL (medial patellofemoral ligament) sits.
Imaging plays a key role in diagnosis. An X-ray shows the position of the kneecap. An MRI scan reveals soft tissue damage, including tears to the MPFL. CT scans help measure the groove depth and alignment. These scans give the surgeon a full picture before recommending treatment.
Non-Surgical Treatment Options
For first-time dislocations without major structural damage, patella instability — Dr Lingaraj advises — often responds well to conservative treatment. This includes:
- Physiotherapy: Strengthening the quadriceps, hip abductors, and core reduces strain on the kneecap.
- Bracing: A patellar stabilising brace helps control kneecap movement during activity.
- Activity modification: Avoiding high-impact sport during recovery allows the ligament to heal.
- Taping: McConnell taping techniques help realign the patella during exercise.
Physiotherapy is central to recovery. At PhysioActive’s physiotherapy services, our team designs structured rehab programmes tailored to each patient’s anatomy and goals.
When Does Dr Lingaraj Recommend Surgery for Patella Instability?
Surgery becomes necessary when conservative treatment fails or when structural problems are severe. Dr Lingaraj identifies three main scenarios that require surgery:
- Recurrent dislocation: The kneecap keeps slipping out despite physiotherapy.
- Significant MPFL tear: The main stabilising ligament is too damaged to heal on its own.
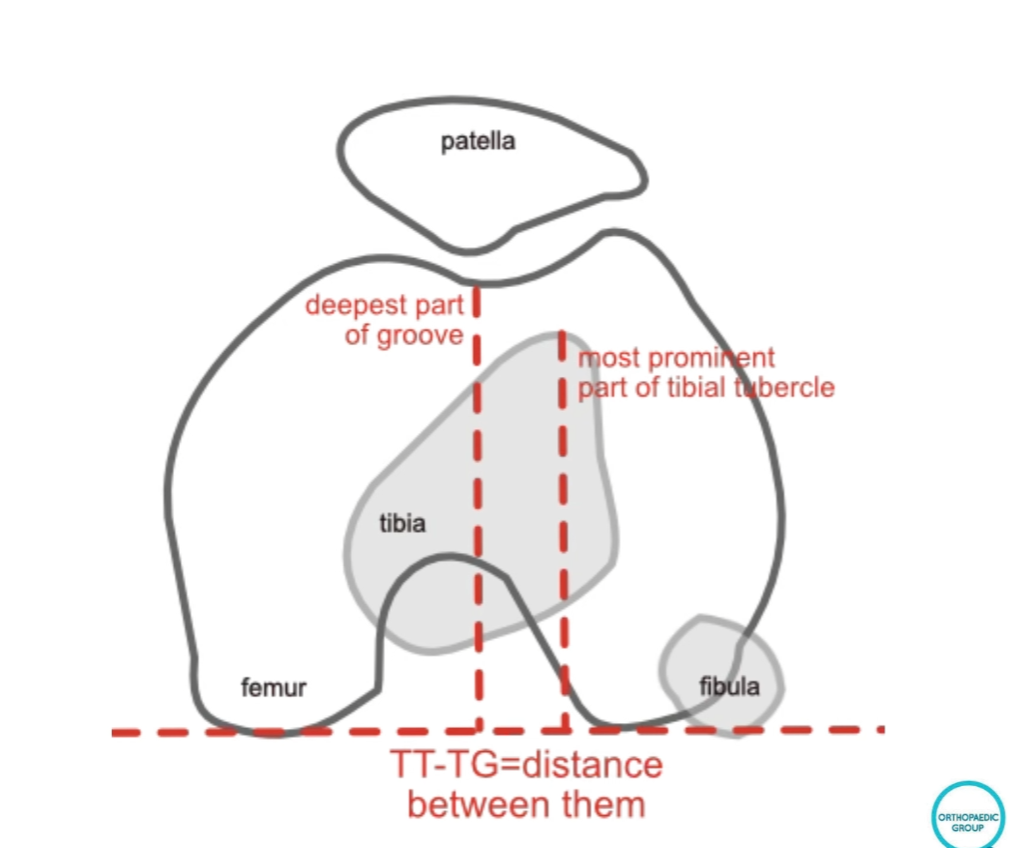
- Bony malalignment: The tibial tubercle is too far to the outside, pulling the kneecap laterally.
According to research published on PubMed, MPFL reconstruction consistently produces good outcomes in patients with recurrent patellar instability. Early surgical intervention — when indicated — reduces long-term joint damage.
MPFL Reconstruction — What Does It Involve?
MPFL reconstruction is the most common surgery for patella instability. The surgeon takes a graft — usually from the hamstring tendon — and uses it to rebuild the torn ligament. This holds the kneecap in place.
Dr Lingaraj performs the surgery under general anaesthesia. Most patients go home the same day or the next morning. The knee requires a brace for the first few weeks. Physiotherapy begins early and continues for several months.
Recovery takes time. Most patients return to sport within six to nine months. Dr Lingaraj is clear with his patients: rushing recovery increases the risk of re-injury. Following the physiotherapy plan closely is essential.
What About Tibial Tubercle Osteotomy?
In some patients, the tibial tubercle sits too far to the outside. This pulls the kneecap laterally and causes instability. In these cases, Dr Lingaraj may recommend a tibial tubercle osteotomy (TTO).
During this procedure, the surgeon cuts the bony attachment point of the patella tendon and moves it to a better position. This corrects the angle of pull on the kneecap. Recovery from TTO takes longer than MPFL reconstruction alone. However, when the anatomy requires it, this procedure gives excellent long-term results.
The Role of Physiotherapy After Surgery
Surgery corrects the structure. Physiotherapy rebuilds function. Without proper rehabilitation, even a well-performed operation may not deliver full results. Dr Lingaraj emphasises this point with every patient.
Post-surgical rehab focuses on three phases:
- Phase 1 (Weeks 1–6): Reduce swelling. Restore range of motion. Activate the quadriceps gently.
- Phase 2 (Weeks 6–16): Build strength in the quadriceps, hamstrings, and hip muscles. Introduce low-impact exercise.
- Phase 3 (Months 4–9): Sport-specific training. Gradual return to full activity.
Our team at PhysioActive works closely with surgeons like Dr Lingaraj to ensure patients receive consistent, structured rehabilitation throughout their recovery journey.
Preventing Future Dislocations
Prevention is always better than surgery. Dr Lingaraj recommends these habits to protect the knee:
- Strengthen hip abductors and quadriceps through regular exercise.
- Wear supportive footwear during sport.
- Use a patella brace during high-risk activities.
- Attend physiotherapy at the first sign of instability — do not wait for a full dislocation.
Early physiotherapy intervention can stop instability from progressing. See a specialist if the knee ever feels like it “wants to give way.”
Ready to Explore Your Treatment Options?
Dr. Lingaraj Krishna
Orthopaedic Surgeon, Singapore
Website: www.drlingarajkrishna.com
Tel: +65 6970 7748 | WhatsApp: +65 8129 1019
PhysioActive Singapore
Website: https://physioactive.sg/
Comprehensive rehabilitation and physiotherapy services
PhysioActive Indonesia
Website: https://www.physioactive.id/
Locations in Jakarta: Darmawangsa, Setiabudi, and Sunter
Expert post-surgical rehabilitation


